
Health data is spread across apps, wearables, cloud systems, telehealth tools, and EHRs, so security now has more points of failure. I’d sum up the research like this: AI helps most with spotting odd behavior early, watching access across systems, and cutting raw data exposure with methods like federated learning and on-device processing.
Here’s the short version:
- Healthcare breaches are a big U.S. problem: 725+ breaches in 2023 exposed 133 million+ records.
- AI helps most with monitoring: it can flag off-hours access, bulk record pulls, strange logins, and odd device traffic and biometric benchmarks.
- Privacy tools matter too: federated learning, differential privacy, and on-device processing can limit where raw patient data goes.
- Wearable data is a special risk: studies cited here report 86% to 100% re-identification rates, even after anonymization.
- AI also adds new risk: model inversion, membership inference, prompt injection, and shadow AI can expose PHI.
- Good security still depends on people and policy: access controls, audit logs, consent tracking, data minimization, and human review still do the heavy lifting.
One stat stands out to me: one Johns Hopkins deployment cut investigation time from 75 minutes to 5 and false positives from 83% to 3%. That shows where AI can help most: not by replacing security teams, but by helping them find trouble faster.
If you use cross-platform health monitoring, the takeaway is simple: use AI for detection, keep data local when possible, and back it all with clear rules and human oversight.
How AI Can Be Used in Healthcare Without Putting Patient Privacy at Risk
sbb-itb-f5765c6
How AI strengthens health data security
AI Health Data Privacy Methods: Federated Learning vs. Differential Privacy vs. Encryption
Recent studies show that AI helps when it watches, sorts, and protects data across systems in real time. It gives teams constant visibility by learning what normal access looks like, then spotting activity that falls outside that pattern across users, devices, and workloads. That includes EHRs, telehealth platforms, cloud systems, and connected devices.
Anomaly detection, behavioral analytics, and continuous oversight
AI security systems build behavior baselines for each user role, such as physicians, nurses, billing staff, and administrators. They track things like usual login times, common locations, access volume, and the types of records each role tends to open.
That matters because odd behavior often shows up before a clear incident does. A clinician logging in from an unusual place at 3:00 a.m. is one thing. The same account pulling a large batch of records it never touches is another.
A Johns Hopkins deployment cut investigation time from 75 minutes to 5 and false positives from 83% to 3%.[12][20]
AI can flag unfamiliar logins, bulk downloads, off-hours access, and suspicious IoMT traffic. From there, it can trigger a lockout, end a session, or send the issue to the SOC for review.[6]
Predictive risk detection and data classification
AI can also spot warning signs that come before ransomware and classify PHI in notes, databases, and live data streams. That gives security teams a way to apply tighter safeguards where the risk is higher, such as MFA, stricter export controls, and stronger encryption.[7][10]
Privacy-preserving methods for cross-platform data use
When data needs to move across institutions or devices, the goal changes a bit. It’s no longer just about spotting threats. It’s also about limiting exposure from the start. A few methods help keep data local while still allowing useful computation.
Federated learning keeps raw patient records at each site and shares only model updates.[8][11] A federated deep learning study published in JMIR AI demonstrated this for lung cancer gross tumor volume segmentation across institutions, showing that clinically useful models can be built without centralizing sensitive imaging data.[3]
Differential privacy adds calibrated noise to model outputs or training gradients, which makes it much harder to reverse-engineer any one person’s data.[9] Research from Google found that federated models with differential privacy can achieve similar accuracy and generalizability to centralized models while offering stronger privacy protections, without significantly raising computational costs.[18]
Wearable and biometric data often need on-device processing. Even short sensor traces - as little as 1 to 300 seconds - can re-identify users.[14]
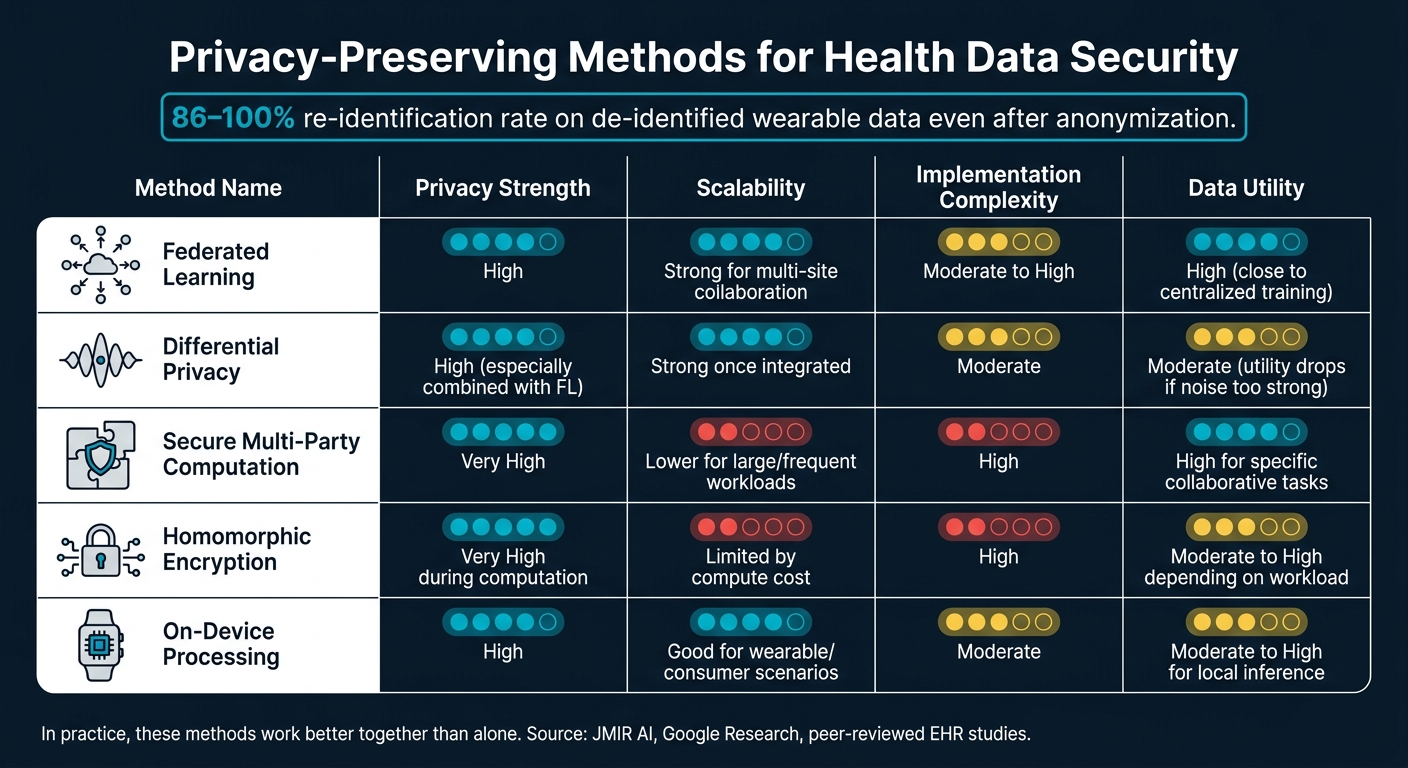
The table below compares the main privacy-preserving methods across a few practical factors:
| Method | Privacy strength | Scalability | Implementation complexity | Data utility |
|---|---|---|---|---|
| Federated learning | High[3][18][1] | Strong for multi-site collaboration[3][18] | Moderate to high[18][1] | High, often close to centralized training[18] |
| Differential privacy | High for output protection, especially when added to FL[18][19] | Strong once integrated into pipelines[18] | Moderate[18][19] | Moderate; utility can drop if noise is too strong[19] |
| Secure multi-party computation | Very high[13][16] | Lower than FL for large, frequent workloads[16] | High[13][16] | High for specific collaborative computations[13] |
| Homomorphic encryption | Very high during computation[15][16] | Often more limited by compute cost[15][16] | High[15][16] | Moderate to high, depending on workload[15] |
| On-device processing | High[14] | Good for distributed consumer/wearable scenarios[14] | Moderate[14] | Moderate to high for local inference, lower for cross-site learning[14] |
In practice, these methods tend to work better together than on their own.
Key risks and limits identified in the research
AI can strengthen health security. But it also creates new ways for things to go wrong. In cross-platform monitoring, each handoff adds risk. Every API, vendor, and device creates another trust boundary, which means another place where data can slip, leak, or get misused.
Data-layer, model-layer, and deployment-layer risks
Researchers usually sort AI-related health data risks into three layers: the data layer, the model layer, and the deployment layer. Each one has its own weak spots and guardrails.
At the data layer, the big risks include poisoning, leakage, and re-identification. If records are corrupted or mislabeled, predictions can drift off course. And if training data is contaminated, models may memorize private details and later reveal them [21][25][29].
At the model layer, two risks stand out: membership inference and model inversion. These attacks can reveal whether a patient's data was used to train a model or piece together private traits from the model's outputs. In plain terms, that can expose someone's link to sensitive care, including mental health or HIV treatment. Research on a Texas hospital discharge dataset found attack accuracy above 70%. On partially synthetic Vanderbilt EHR data, 82% of individuals were identified as training-set members at 0.9 precision [24][28][33][35].
At the deployment layer, risk comes from the way generative AI gets plugged into day-to-day systems. Prompt injection can push an EHR-connected assistant to reveal PHI or take unauthorized actions [23][25][27]. Shadow AI can create data flows that sit outside normal governance and leave no clear record behind [30][32]. That's why access control, audit logs, and continuous monitoring matter so much here.
Why wearable and biometric data streams need extra safeguards
Continuous biometric streams create more than a storage problem. They create a steady inference problem. High-frequency signals like heart rate, accelerometer readings, sleep patterns, and electrodermal activity build up over time into a detailed picture of daily life, stress, and health status [22][26][31].
The re-identification issue is especially severe. Studies on de-identified wearable sensor data report correct re-identification rates of 86–100%, even after anonymization [34][36]. So if de-identification sounds like a fix on paper, the research shows it often falls short in practice.
The U.S. setting makes this even tougher because of a gap in oversight. Most consumer wearables sit outside FDA medical-device rules and HIPAA unless they're used in clinical care [26][31]. As a result, personal signals like sleep disruptions, stress spikes, and irregular heart rhythms can often be collected and reused by third parties [26][31]. Once AI is layered on top of that data to infer mood, behavior patterns, or mental health status, the privacy risk gets even higher [37].
Governance, compliance, and trust in AI health security
Access controls, audit logs, and compliance monitoring
Risks in AI health systems don’t sit in just one place. They show up in the data, the model, and the way the system is used in practice. That’s why governance has to cover all three.
At its core, governance turns security policy into rules people and systems have to follow. Research and compliance guidance tie better results to RBAC, least privilege, audit logs, retention limits, and data minimization.[45][38][43] In plain English, that means only approved staff or systems can access protected health information, every access event is recorded, logs stay available long enough for review, and the system gathers only the data it needs.
Use role-based masking so each user sees only the fields required for their job.[48] For AI systems, the audit trail should show:
- Which person or system accessed PHI
- What action was taken
- Which data was touched
- Who approved the access[4]
OCR treats audit logging and monitoring as HIPAA safeguards, and HITRUST adds specific rules for log content, review timing, and centralized monitoring.[49][38][43]
Consent tracking and retention rules fill in the rest of the picture. If an organization can show what a user approved, how long data is kept, and when it is deleted, it becomes much easier to prove compliance during an audit.[41][42]
How transparency affects user trust and adoption
Compliance is only one piece of the puzzle. Transparency plays a big part in whether people trust the system enough to use it.
CHAI survey data make that pretty clear: 51% of respondents say AI makes them trust healthcare less, only 12% say it increases trust, and 93% report at least one concern about AI use in health care.[51]
Research on AI in health care shows that when patients are told how AI is being used, trust goes up for both the provider and the AI system.[46] The practices that seem to work best are simple ones: plain-language disclosures, clear consent, and easy delete/export controls, especially when data moves across apps, devices, and systems.[39][40][44]
People shouldn’t have to guess. They need to know what is collected, who can see it, and how to change it.
A practical note for consumer health apps such as Healify
These governance lessons matter just as much for consumer health apps. In many cases, wearable and biometric data sit outside HIPAA unless they are used in clinical care.[47][50] That creates a gap. The data may feel as sensitive as medical data, even when the law treats it differently.
For an app like Healify, which continuously analyzes wearables, biometrics, bloodwork, and lifestyle data from many sources to deliver personalized coaching, that points to a few clear moves: plain consent at onboarding, simple in-app delete/export controls, and privacy-preserving processing where possible.[41][42][47][52]
A systematic review of privacy policies across 17 leading wearable manufacturers found major gaps in transparency, data minimization, and user control.[52] Consumer health tools should fix those gaps by default. Governance isn’t just a back-office task. It shapes whether people feel safe handing over deeply personal health data.
These controls work best as part of a layered defense.
What the evidence supports most strongly
A layered defense approach for cross-platform health monitoring
When you put these studies side by side, one point stands out: there isn't one magic fix. Health data doesn't stay in one place. It moves across devices, apps, wearables, and clinical systems. That makes security a system-wide job, not a single-tool job.
The research leans toward a layered defense model: encryption, IAM, AI monitoring, federated or on-device processing, and predeployment red-teaming.[60][5]
These controls do more when they work together. On their own, each one helps. As a group, they cover more ground.
Current gaps in the literature
That said, a lot of the upside comes from narrow studies, not broad rollout data. Most of the evidence comes from simulations, short pilots, or single-site datasets. Long-term, multi-hospital studies are still rare.[17][11][58]
Interoperability is still a major pain point. In day-to-day U.S. healthcare settings, teams often deal with fragmented EHR systems, legacy devices, and uneven data formats. So while controlled studies can look promising, putting those same controls into practice is often messier than it seems on paper.[56][57][59]
There are also weak spots in AI-focused defense. Protections against model inversion, membership inference, poisoning, and attacks enabled by generative AI are still immature.[53][56][11]
Key takeaway
Even with those limits, the pattern is pretty clear. The strongest evidence backs AI for early threat detection and continuous oversight.[60][5][2] It also backs privacy-preserving methods like federated learning, which can help systems work with shared data without pulling raw records into one central store.[61][3][62]
What AI does not do is replace human governance, clear policy, or a well-engineered security stack underneath it.
For consumer health apps like Healify, which process wearable, biomarker, bloodwork, and lifestyle data, the practical move is simple: limit raw data exposure whenever possible. In practice, that means leaning on on-device processing, federated analytics, strong IAM, clear consent, and human-led oversight of how the AI behaves over time.[54][55][8]
AI can help spot problems early. But the way the system is built - and the rules behind it - decides whether people can trust it.
FAQs
How does AI detect health data threats early?
AI helps detect threats to health data early by scanning for unusual activity in real time. That means it can flag spoofed devices, forged data, unauthorized network attacks, and system weak points like hardcoded secrets or known software flaws.
It can also log sensitive API activity to create secure, unchangeable audit trails. In plain English, that gives teams a clear record of what happened and when, so they can respond fast and protect data as it moves from wearable sensors to healthcare providers.
Why is wearable data hard to anonymize?
Wearable data is tough to anonymize because it’s highly specific and packed with detail. These devices record sensitive, long-term information such as heart rate patterns, sleep cycles, and GPS history. Even if you strip out names and other direct identifiers, that data can still form a clear personal profile.
There’s another problem too. Wearables track movement and physical responses in real time, so the context is often what makes the data useful. Take too much of that context away, and the clinical use of the data starts to drop.
What security controls still matter beyond AI?
AI can help. But it doesn’t replace the basics.
If you’re protecting health data, core security controls still matter. That means strong access management with unique user IDs, multi-factor authentication, solid password habits, and regular firmware and software updates.
There’s also the vendor side of the equation. Organizations still need Business Associate Agreements (BAAs) with third-party vendors. And when it comes to data protection, trusted technical standards still do the heavy lifting: AES-256 for data at rest and TLS 1.2+ for data in transit.