
Wearables are turning telemedicine from a one-time video visit into care that runs between visits. In this article, I’d sum it up like this: the data matters, but the system around the data matters more. If clinics want to use smartwatch, CGM, ECG patch, and smart ring data well, they need AI triage, clean data standards, alert rules, EHR handoff, privacy controls, and an easy patient setup.
Here’s the short version:
- Continuous data fills gaps that a 15-minute visit can’t show
- AI helps sort high-volume readings so care teams don’t drown in numbers
- FHIR and clean mapping help move data into the EHR with context intact
- Remote monitoring is growing fast, with Medicare RPM claims up 555% from 2019 to 2022 in one cited source
- Workflow and consent are just as important as the device itself
- Patient drop-off often starts with setup friction, like pairing, apps, and syncing
A few numbers stand out:
- About 3 in 5 U.S. adults now own a wearable or connected health device
- A CGM can generate 288 readings per day
- A 500-patient RPM program can create 5,000 to 7,500 data points daily
Wearables, remote patient monitoring & the future of chronic care management with Richard Milani, MD
sbb-itb-f5765c6
Quick take
If I were reading this to get the answer fast, here’s what I’d want to know:
| Area | What’s changing | Why it matters |
|---|---|---|
| Data flow | Device → app/cloud → normalization → dashboard → EHR | Bad handoffs make the data hard to use |
| AI triage | Systems sort high-risk signals first | Cuts clinician review time |
| Interoperability | FHIR APIs and source tagging | Keeps timing, units, and device context clear |
| Remote monitoring | Use is moving past high-risk care | Supports follow-up, sleep, stress, and prevention |
| Privacy | HIPAA, consent, provenance, revocation | Builds patient and clinician trust |
| Patient experience | Less setup friction, clearer feedback | Helps people keep using the device |
So if you want the plain-English takeaway, it’s this: wearable data only helps when it reaches the right clinician, in the right format, at the right time, with clear patient permission. The rest of the article explains where that process works, where it breaks, and what care teams should watch next.
How wearable data moves from device to clinical decision
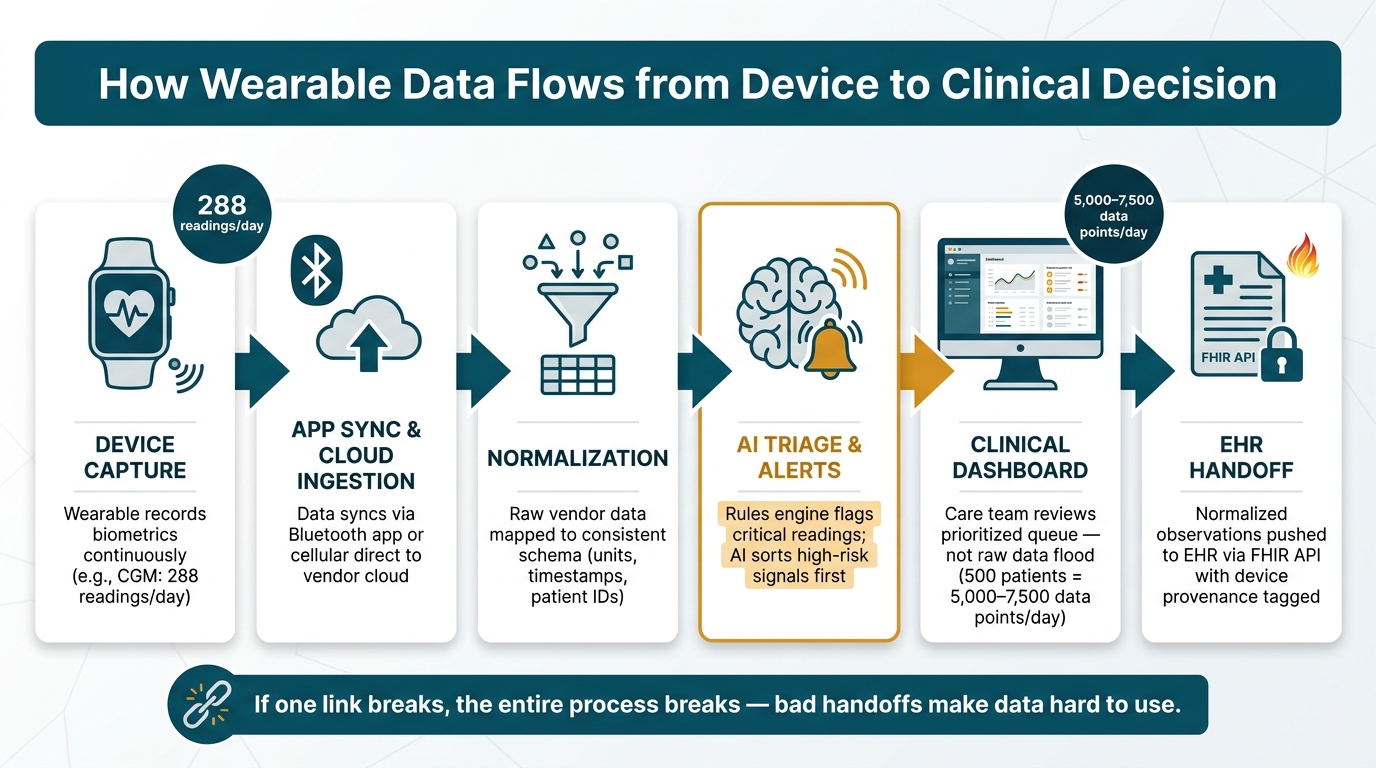
How Wearable Data Flows from Device to Clinical Decision
Wearable data gets to clinicians through a pretty fragile chain: capture, sync, normalization, and review. If one link breaks, the whole process gets messy. And that’s exactly where many of today’s big shifts are showing up.
Device capture, app sync, and cloud ingestion
A lot of wearables sync over Bluetooth to a companion app. That health AI app stores data on the phone and then sends it to the cloud in the background [6][7]. This matters because users don’t have to keep tapping buttons or manually uploading files. Data keeps moving on its own, and that steady flow is what makes remote review possible.
Some cellular wearables cut out the phone entirely and send data straight to a vendor cloud. That sounds simpler, and in some cases it is, but there’s a tradeoff: it ties the workflow more tightly to the vendor’s APIs [7].
Once the data lands in the cloud, the next step is harder than it sounds. Clinicians can’t do much with raw device output unless it’s turned into something clean and usable.
Normalization, dashboards, and alerts
Raw vendor data almost never shows up in a format a care team can use right away. Without normalization, clinicians end up looking at noisy readings instead of observations they can act on. So the data has to be mapped into a consistent schema before it can show up on a clinical dashboard [6][7].
After that, a rules engine can flag readings that need attention, like extreme heart rate, blood pressure, SpO2, or glucose values, and send them to the right place based on urgency [7]. That filtering step is a big deal. Even small remote monitoring programs can produce thousands of readings per day [7].
Without normalization, clinicians see noisy device output instead of reliable observations.
That’s why the dashboard shouldn’t just show more data. It should show the right data, with enough structure to help a clinician make a call fast.
EHR handoff and care team review
Once observations are normalized and filtered, they can be pushed into the EHR through standard APIs. Each observation should include device provenance so clinicians know where it came from [7]. It also helps to tag readings at the ingestion layer by source, whether they came from a consumer device or a medical device [6][7].
A simple way to think about it:
- Use the EHR for summarized observations and clinical decisions
- Use the telehealth platform for real-time triage and review [3]
That split keeps the EHR from turning into a dumping ground for raw device feeds. The point isn’t to stuff more data into the record. The point is to send cleaner data that helps the care team decide faster.
With the path laid out, the next issue is how AI, interoperability, and workflow design turn that stream of readings into something a clinic can use day to day.
The biggest trends shaping wearable data integration
AI is turning raw data into actionable signals
The main issue isn't a lack of data. It's the flood of it.
Wearables produce far more information than clinicians can reasonably review on their own. AI helps sort that stream by spotting the patterns that matter - like blood pressure that stays high or signs of atrial fibrillation - before those readings ever hit a clinician's dashboard [9][4]. Predictive analytics can also catch small changes in resting heart rate and body temperature that may point to illness before symptoms show up [9].
That changes the day-to-day experience for care teams. Instead of dealing with a nonstop stream of numbers, clinicians get a queue shaped around priority.
Generative AI is also starting to show up inside wearable platforms themselves. It can turn raw biometric data into plain-language summaries and suggest AI-driven treatment plans based on the person's readings [9][5].
"The promise of remote patient monitoring will remain largely unfulfilled until AI-driven triage layers are widely available to sift through wearable telemetry." - Julia Lainster, HealthTech Solutions Expert [9]
Even so, better signal detection only gets you so far. If one system reads the data one way and another reads it differently, the handoff breaks down fast.
Interoperability is now a requirement, not a bonus
The tougher problem isn't just getting data from one place to another. It's making sure the meaning stays intact along the way.
Wearable makers still use different data formats, and many still keep users inside closed ecosystems [4]. Without semantic alignment - shared units, timestamps, and patient identifiers - data can land in the EHR as unmapped entries stripped of context [1]. That's a big deal. If a blood pressure reading shows up without clear timing or source details, it's much less useful in care.
FHIR-based APIs are now the closest thing the market has to a common standard. They map device output into structured resources like Observation and DeviceMetric, which gives EHRs something they can actually work with [4][1].
"At scale, the hardest part of wearables is not moving bytes. It is preserving meaning, trust, and timing from the patient's wrist, patch, or ring all the way to the EHR." - Behind.cloud [1]
The business side tells the same story. RPM claims grew by nearly 1,294% between 2019 and 2022 [3], and that kind of growth depends on a data pipeline that can stand up to documentation rules.
When that structure is in place, wearable data can do much more than support chronic care.
Remote monitoring is expanding beyond high-risk care
Wearable integration isn't just for high-risk patients anymore.
The same setup now supports post-discharge follow-up, preventive wellness, sleep tracking, and stress monitoring - areas of care that barely had steady, continuous data options a few years ago [3][1].
There's a simple reason this matters: steady wearable use creates long-term, day-to-day health records from real life, not just snapshots from clinic visits. That gives clinicians something they've rarely had before. And because the readings happen outside the exam room, they can reduce the white coat effect, when vitals rise during appointments, which helps providers see a more accurate baseline [4].
The bigger shift here is from reacting to problems after they show up to stepping in earlier, when the first signs appear. That puts more pressure on workflow design, privacy controls, and patient participation.
What healthcare teams and patients need for wearable data to work
Clinical workflows must prevent data overload
Once wearable data reaches the clinic, the hard part changes. It’s no longer about gathering readings. It’s about sorting them fast enough to help, not swamp, the care team.
The main bottleneck is workflow, not collection. A single RPM patient using more than one device can produce 10–15 readings a day. In a practice with 500 patients, that turns into 5,000–7,500 data points every day [7]. Without a smart filtering layer, that flood of information can bury clinicians instead of helping them.
One of the best ways to handle that volume is tiered alerting. Instead of dumping every reading into one queue, custom dashboards with tiered alerts should route data based on urgency. Critical readings should go out right away, urgent ones within an hour, and routine trend data should land in daily digests. Edge filtering can also trim noisy data before it even reaches the cloud.
Another piece matters here: physiological plausibility checks. If a system sees something impossible - like a systolic blood pressure of 500 mmHg - it should flag that reading before it reaches the clinician or gets auto-filed into the EHR [7].
"RPM does not create value from more data. It creates value from a better signal." - Mindbowser [10]
Privacy, security, and consent build patient trust
Once data is triaged, it still has to move into the clinical record in a secure, trackable way. The moment wearable data travels from a device to a clinician platform, it becomes protected health information, or PHI, under HIPAA [2]. So transmission, storage, and access need to be handled with the same care as any other part of the medical record.
Each EHR entry should also show provenance - the device, platform, and transfer path behind the reading - so there’s a clear trail for every data point [7]. Secure integration depends on that recordkeeping, plus unique device IDs and a plain revocation process for devices that are lost or compromised [1].
Consent is just as important. Patients should clearly approve data sharing from their devices to clinical apps, and they should have a clear way to revoke that access if needed [8][1]. People tend to stay involved when they know who can see their data and how that access can be turned off.
Trust on the clinical side is shaped by FDA status too. Pathways like 510(k) clearance, Premarket Approval (PMA), and De Novo classification help separate medical-grade data from general wellness metrics [5].
"A device that is cleared or approved by the FDA is worth a physician's attention... but that may not be true for devices without FDA clearance or approval." - Jared Dashevsky, MD [5]
Patient experience determines long-term engagement
Security by itself won’t keep people using a device. The experience also has to feel easy enough to stick with. And in many cases, the first thing that gets in the way is setup.
Bluetooth pairing, app downloads, and manual syncing sound small on paper. In practice, they create real friction. Cellular-connected devices avoid a lot of that by sending data straight to the cloud, with no smartphone needed [7]. That kind of plug-and-play setup also helps patients who have trouble with smartphone use or broadband access.
People are also more likely to keep going when the system tells them what the numbers mean and what they should do next. Raw readings, on their own, can feel like noise. But when a platform turns biometric trends into clear, personal guidance, the data starts to feel useful instead of confusing.
"Technology adoption in healthcare happens when systems reduce clinician effort, not when they add new dashboards." - Mindbowser [10]
The same idea holds for patients. Wearable programs with the strongest long-term participation make the experience feel simple and worth the effort - not like one more task hanging over the day. The systems that work best turn steady streams of readings into clear next steps.
Conclusion: What to watch next in wearable-enabled telemedicine
Wearable data integration is moving past simple data collection. Now the focus is orchestration. The big question is no longer who can gather the most signals. It’s which systems can turn those signals into timely action.
In practice, that means a shift in care delivery toward proactive monitoring for chronic diseases. Instead of waiting for symptoms to get worse, care teams can spot changes early and send those signals straight into clinical workflows.
But detection alone won’t decide who scales. Two things matter most here: interoperability and AI filtering. The systems that stand out will show clinicians only the signals that need attention and send them to the right person at the right time.
The same idea applies to patients. Wearable-enabled telemedicine now depends on one thing above all else: turning signals into action. Tools like Healify point in that direction.
FAQs
How can clinics avoid alert fatigue from wearable data?
Clinics can cut alert fatigue by moving away from static thresholds and using AI-powered filtering instead. Rather than relying on one-size-fits-all limits, they can use personalized patient baselines. That helps the system flag changes that actually matter, not short-lived artifacts or noise.
They can also use data pipelines to sort alerts by urgency. In practice, that means separating alerts that need immediate escalation from signals that point to longer-term trends. At the same time, automated filtering can lower clinician cognitive load and make the alert stream easier to act on.
What wearable data should go into the EHR?
Clinically relevant wearable data for the electronic health record (EHR) includes continuous metrics that help with chronic disease management, remote monitoring, and diagnostic decisions.
This usually covers heart rate and rhythm, blood oxygen saturation (SpO2), glucose, body temperature, blood pressure, and weight. It also includes activity, sleep, and stress data.
For clinical use, these data streams are usually standardized as FHIR Observation resources before they’re integrated into the EHR.
How do patients give and revoke data-sharing consent?
Patients usually handle data-sharing consent through their device’s built-in permission tools, such as Apple HealthKit or Google Health Connect.
In an app like Healify, you can allow or remove read and write access for specific health data types in your device settings. You can check or update these permissions anytime in your phone’s privacy settings.