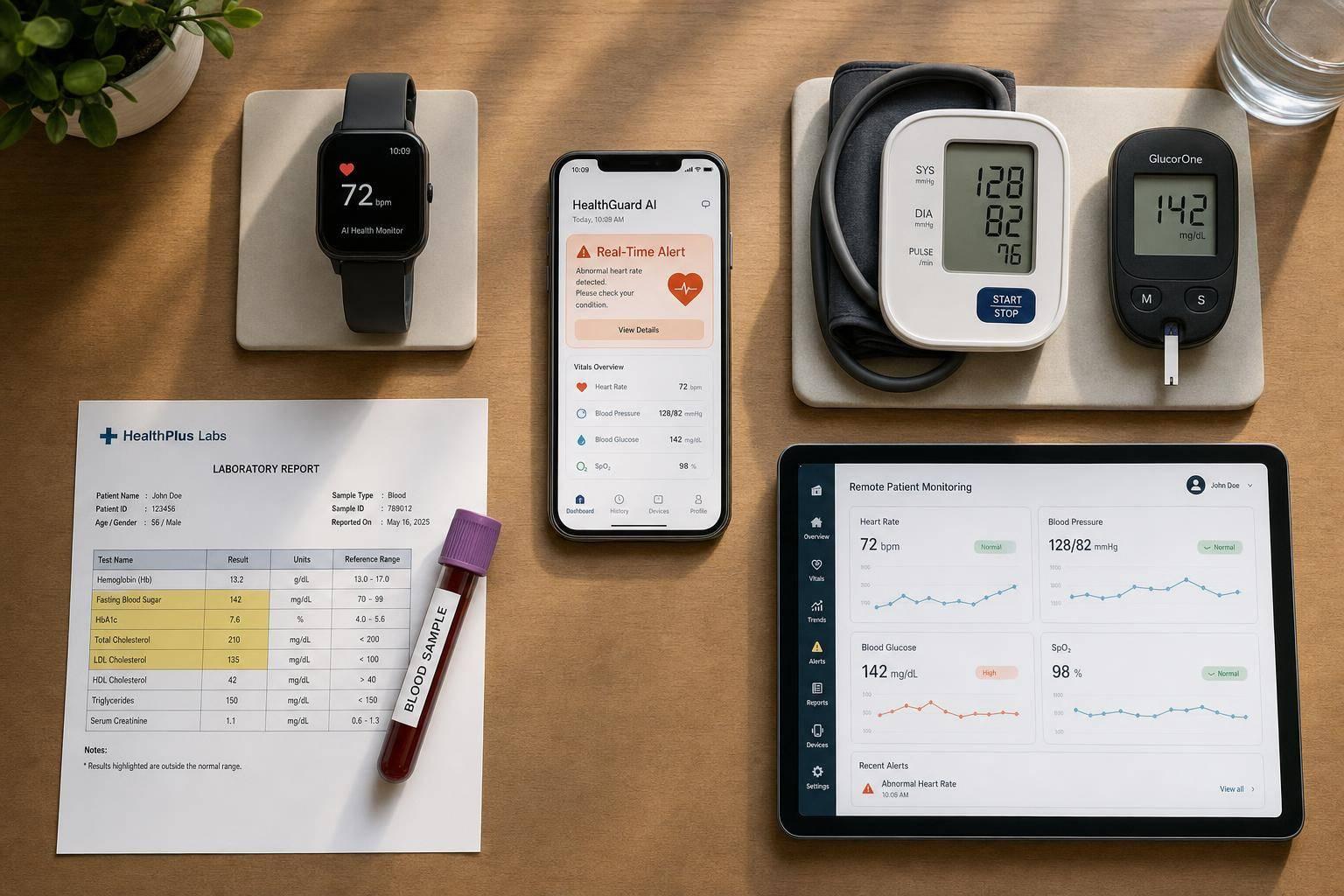
If you want the earliest warning, AI wearables lead. They watch data all day, can flag risk within seconds, and in some cases warn hours before a health event. But if you want cleaner clinic workflow, home devices, RPM, and office testing still have a big role.
Here’s the short version:
- AI-integrated wearables are best for early warning and multi-signal pattern detection
- Non-AI wearables are good for basic tracking, but they usually alert only after a number crosses a set limit
- Connected home devices work well for blood pressure, weight, glucose, and oxygen checks taken at home
- Clinic-based monitoring is best for diagnosis and treatment decisions, but it misses changes between visits
- Standard RPM programs help care teams watch home readings between visits, though alerts depend on patient use and staff review
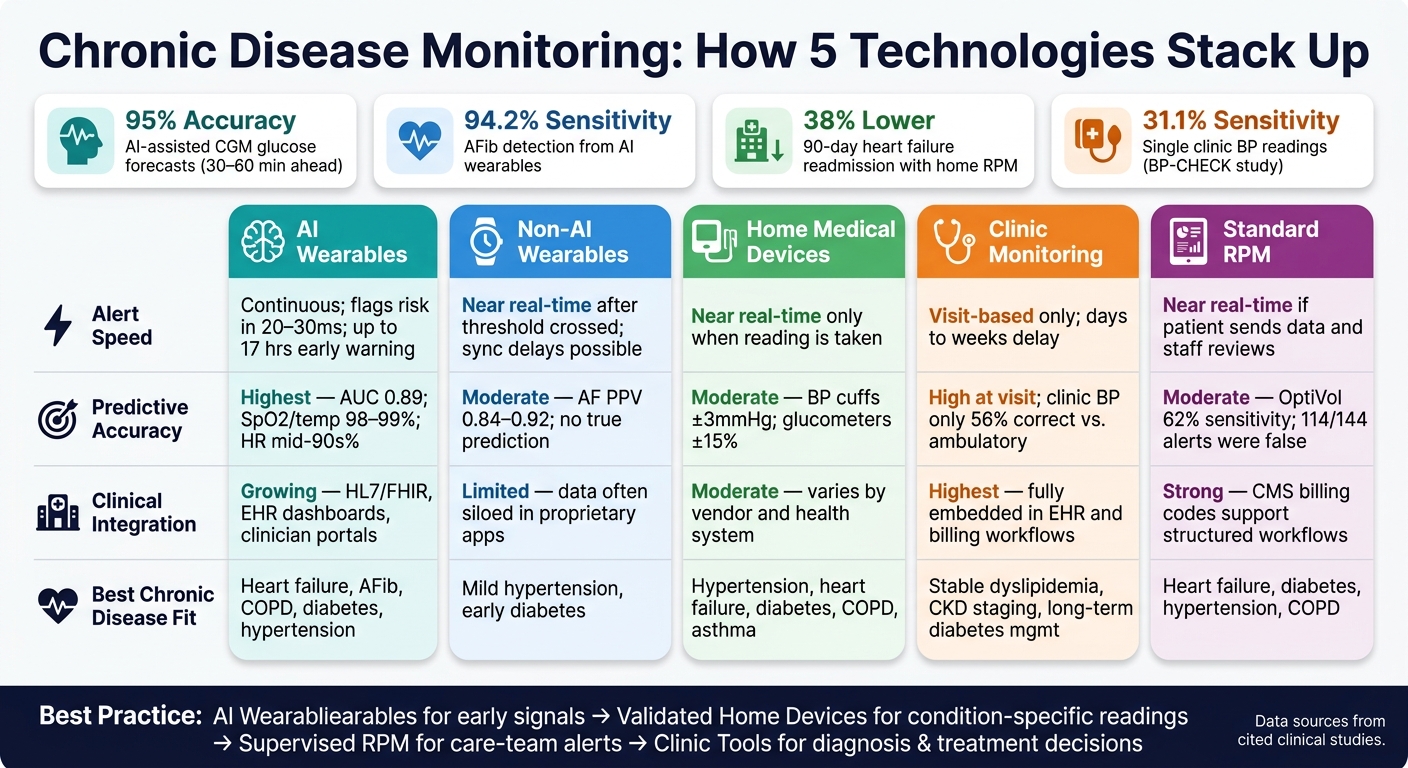
A few numbers stand out:
- AI-assisted CGM has been reported at about 95% accuracy for 30–60 minute glucose forecasts
- AFib detection from AI wearables reached 94.2% sensitivity and 95.3% specificity
- Heart failure RPM programs using home devices were linked to a 38% lower chance of 90-day readmission in one cited result
- Single clinic blood pressure readings showed only 31.1% sensitivity in the BP-CHECK study
AI Wearables vs. Home Devices vs. Clinic Monitoring: Chronic Disease Alert Comparison
S7E3 | Using Wearables and AI to Detect Disease Earlier | The Health Pulse Podcast
Quick Comparison
| Option | How fast it alerts | What it does best | Main limit |
|---|---|---|---|
| AI wearables | Continuous; can flag risk early | Spots patterns across many signals | Device fit, motion noise, privacy, battery |
| Non-AI wearables | Near real time after threshold is crossed | Simple tracking for one metric | Little to no prediction |
| Home medical devices | Fast only when a reading is taken | Good for BP, weight, glucose, SpO2 | Gaps if the patient skips checks |
| Clinic monitoring | Slow; visit and lab based | Diagnosis and confirmatory testing | No between-visit warning |
| RPM programs | Near real time if data is sent and reviewed | Structured care-team follow-up | Staff workload and alert volume |
My takeaway: if your condition can change fast - like diabetes, heart failure, AFib, or COPD - continuous monitoring usually gives you a better shot at catching trouble early. But the best setup is often a mix: wearables for early signals, home devices for checked readings, and clinic tools for diagnosis and treatment changes.
Below, I break down where each option fits, where it falls short, and what those trade-offs mean for day-to-day care.
1. AI-Integrated Wearable Sensors
The big advantage here is latency. With continuous sensing paired with analytics, these devices can flag risk in 20–30 milliseconds.[5][4] Alerts can go to both the patient and the care team at the same time.[8][9][13][16] So when you judge these systems, the first thing to look at is simple: how fast do they react?
Alert Timeliness
These sensors can catch atrial fibrillation, oxygen drops, or fast glucose swings within seconds.[5][8][4][12][13][6] That speed comes from adaptive thresholds that compare new readings against each patient’s usual baseline. In plain terms, the system is not just looking for a bad number. It’s looking for a bad number for that person. That helps cut down on false alarms while keeping the alerts fast.
Predictive Accuracy
The reported numbers are strong. SpO₂ and temperature accuracy can hit 98%–99%. Heart rate accuracy sits in the mid-90% range. AFib sensitivity reaches 94.2% with 95.3% specificity. And AI-assisted CGM can predict glucose levels 30–60 minutes ahead with about 95% accuracy.[4][12]
That said, performance still depends on the sensor itself and how well it fits. If the hardware is lower grade, or if motion artifacts interfere with the signal, accuracy can slip. Consumer devices can fall short of medical-grade systems for that reason.[11][13]
And this is where the point gets practical: high accuracy only helps if the data gets to clinicians fast enough to affect care.
Clinical Integration
These sensors do their best work when they plug into clinical workflows instead of sitting inside a consumer app alone. In most setups, wearable data is mapped into HL7 or FHIR and then shown in EHR dashboards or remote monitoring workflows.[7][11][14]
Many teams start small. A pilot in one specialty - often cardiology or endocrinology - is a common first step. That gives the care team room to tune alert thresholds and tighten escalation protocols before a broader rollout.[13][15] Patient-facing apps can also pull together wearable data, bloodwork, and lifestyle inputs so alerts lead to day-to-day action, not just another notification.[10][17]
Chronic Disease Fit
The best use case is pretty clear: conditions where a steady, non-invasive signal maps well to risk over time.
A 2025 review of 60 studies found that most AI wearable research focused on type 2 diabetes, where CGM data helps predict glycemic excursions.[18] Cardiovascular conditions come next, including heart failure, AFib, and hypertension. After that, chronic respiratory diseases like COPD stand out, since wearables that track respiratory rate, SpO₂, and activity can catch signs of an oncoming exacerbation early enough for care teams to step in.[5][4][13][6]
That’s why these conditions line up so well with wearables: they reward early pattern detection.
2. Non-AI Wearable Devices
If AI-integrated sensors set the bar, non-AI wearables are the simpler starting point: fast at spotting problems, limited when it comes to seeing them ahead of time. These devices run on fixed thresholds. A CGM sends an alert when glucose moves past a preset limit. A smartwatch flags an elevated resting heart rate. That difference matters when you compare them with AI-integrated systems.
Alert Timeliness
For threshold-based events, alerts can arrive near real time. A CGM can notify a patient almost as soon as a glucose low is detected. An ECG patch can flag a rhythm change as it happens. But there’s a catch: these alerts fire only after the threshold has already been crossed. Bluetooth issues or phone-sync gaps can also delay or block them.[21][25]
Predictive Accuracy
For narrow, clearly defined tasks, non-AI wearables perform reasonably well. The Apple Heart Study found that 84% of irregular pulse notifications matched confirmed atrial fibrillation, and 34% of notified participants had AF confirmed by follow-up ECG patch monitoring.[19] A Circulation Research review reported a positive predictive value of 0.84 to 0.92 for AF detection from irregular pulse notifications across large smartwatch studies.[26]
Those numbers make a solid case for screening. Prediction is another story. A device that spots an issue after it appears is not doing the same job as one trying to estimate risk before the event.
One caveat matters here. The FDA has warned that smartwatches or smart rings claiming blood glucose measurement without skin penetration are not authorized, cleared, or approved.[29] Any smartwatch or smart ring making a noninvasive blood glucose claim should be treated as unverified. The FDA has not authorized, cleared, or approved those claims.
Clinical Integration
Integration quality is all over the map. FDA-cleared devices such as AliveCor's Kardia Mobile for ECG monitoring or Dexcom's Stelo, the first over-the-counter wearable glucose biosensor cleared in 2024, can fit into care workflows.[28][30] Consumer apps often keep data inside their own systems, with sharing handled manually during visits or through exported reports.[23][24]
For chronic disease care, FDA clearance and EHR connectivity matter more than the name on the box.
Chronic Disease Fit
Non-AI wearables work best when one continuous metric leads straight to an action. That’s the case with diabetes, arrhythmia, and COPD oxygen monitoring.[27][22] They have a harder time when risk depends on several signals at once.
When monitoring calls for more than one signal, connected home devices become the next step.
3. Connected Home Medical Devices
Connected home medical devices sit in the middle ground between clinic equipment and wearables. Think Bluetooth blood pressure cuffs, Wi-Fi scales, connected glucometers, pulse oximeters, and smart inhalers. These tools send readings to an app, cloud platform, or clinician dashboard. The tradeoff is pretty simple: you give up continuous sensing, but you get easier setup and broader use at home.
Alert Timeliness
Alerts here are near real-time, but only when a reading is taken. That matters.
A heart failure patient who steps on a connected scale every morning can trigger an immediate alert to their care team after gaining 2–3 lb in 24 hours or 5 lb in a week. That can be fast enough for a same-day medication adjustment.[31][38] But there’s an obvious catch: if the patient skips that morning weigh-in, nothing gets flagged.
Predictive Accuracy
Accuracy depends a lot on two things: whether patients use the device regularly and how the data gets interpreted in the analytics layer.
FDA-cleared devices are clinically reliable when used the right way. That includes validated blood pressure cuffs within ±3 mmHg and glucometers within ±15%.[32][37] The bigger issue is what happens after the reading comes in. Many programs still lean on simple threshold rules instead of models that look at more than one signal. And that can leave blind spots.
A single metric, like weight or blood pressure, doesn’t always tell the whole story. Programs that add AI-driven risk stratification on top of home-device data tend to spot decline earlier because they look for patterns across several signals at once, instead of waiting for one number to cross a preset line.[35][38]
Clinical Integration
With these devices, the main problem usually isn’t sensing speed. It’s whether the reading gets to the care team fast enough for someone to act on it.
Home-device platforms can now push readings into EHR charts, but that only helps when escalation rules are clear. In practice, teams still run into friction:
- data overload
- interoperability gaps between device makers
- unclear escalation protocols
Any one of those can slow clinical response, even when the data is already there.[36]
Chronic Disease Fit
These devices work best when one reading can directly affect care. That makes them a strong fit for hypertension, type 2 diabetes, heart failure, COPD, and asthma.
Remote monitoring programs that use home weight scales, blood pressure cuffs, and pulse oximeters have been linked to a 38% lower likelihood of heart failure-related hospital readmission within 90 days compared with usual care.[33] Smart inhalers like the Hailie sensor add another layer by tracking every actuation - time, date, and location - to flag adherence gaps in asthma and COPD. That matters because, in asthma, fewer than 50% of patients adhere to preventive medications.[34]
Where connected home devices start to struggle is with conditions that need continuous, high-frequency monitoring. Arrhythmia detection, seizure prediction, and subtle autonomic changes are good examples. In those cases, episodic home measurements just can’t keep pace with continuous wearables when the goal is fast detection of sudden change.
sbb-itb-f5765c6
4. Clinic-Based Diagnostic Monitoring
When home readings are too thin or all over the place, clinic testing becomes the backup plan. This is the classic model: the patient comes in, gets tested, and the results go into the EHR. That usually includes lab work such as HbA1c, lipid panels, creatinine, and eGFR, along with device-based tests like 12-lead ECGs, spirometry, and echocardiograms. It’s built for scheduled confirmation, not round-the-clock tracking.
Alert Timeliness
This is the biggest weak spot for clinic-based monitoring. Alerts show up only during visits or when lab results come back, often days or even weeks after a patient starts getting worse. A patient with hypertension may have blood pressure checked only in the office, which can miss spikes between visits. In heart failure, decline is often noticed only after symptoms like weight gain, dyspnea, or edema push the patient to come in, instead of being flagged by early physiologic signs.
Predictive Accuracy
Clinic-based tests are highly reliable when they’re used the right way, but a single office reading can still point care in the wrong direction. The BP-CHECK study found that single clinic blood pressure readings had 31.1% sensitivity and 79.5% specificity, missing hypertension more than half the time.[40] A BMJ analysis found that, compared with ambulatory monitoring, a clinic-based hypertension diagnosis was correct only about 56% of the time.[41]
For diabetes, clinic HbA1c testing every 3–6 months helps with long-term trend tracking. But it can’t warn clinicians about an acute hypoglycemia episode the way continuous glucose monitoring can.[43]
Clinical Integration
This is where clinic-based monitoring does best. Lab results, imaging, and device data already move into EHRs alongside medications and clinical notes. Billing and reimbursement paths are already in place too, with CPT codes and Medicare coverage covering most in-clinic diagnostics. That setup gives clinic-based monitoring a clear edge when it comes to standardization and workflow fit.
Chronic Disease Fit
Clinic-based monitoring works best for conditions where scheduled, high-quality measurements guide treatment decisions. Good examples include:
- stable dyslipidemia
- CKD staging
- long-term diabetes management
It works less well for conditions that change fast and unpredictably, such as brittle diabetes, frequent COPD exacerbations, or advanced heart failure. In those cases, waiting until the next appointment can mean missing the window to step in.
That gap is why standard remote patient monitoring exists: it extends clinic oversight between visits.
5. Standard Remote Patient Monitoring Programs
Clinic testing gives you snapshots. RPM fills in the time between those snapshots. Standard remote patient monitoring programs use connected readings from home to spot risk between visits. If a reading passes a preset cutoff - like blood pressure above 140/90 mmHg - the system sends an alert to the care team.
Alert Timeliness
Critical alerts often appear within minutes, but there’s a catch: that only happens after the patient takes a reading and someone reviews it. So the speed of RPM depends on two simple things:
- Did the patient send the data on time?
- Was a nurse or care coordinator available to respond?
If either step slips, the alert does too.
Predictive Accuracy
Standard RPM is built to catch what’s happening now, not what may happen next. It flags threshold breaches in the moment.
That limit shows up clearly in heart failure monitoring data. A conventional heart failure monitoring system, OptiVol, showed 62% sensitivity for detecting HF hospitalizations, but it also produced 114 false alerts out of 144 total alerts.[33]
Some RPM programs add prediction on top of the usual threshold rules, and those results look stronger. One heart failure algorithm gave a median advance warning of 34 days before HF events, with 70% sensitivity and few unexplained alerts.[33] So by default, RPM is still threshold-based, with prediction added only in some setups.
Clinical Integration
When RPM data flows straight into an EHR, clinicians can check home trends next to medications, labs, and visit notes in the same place. That means home monitoring becomes part of the day-to-day clinical workflow between visits instead of sitting off to the side.
That setup can matter in practice. Across 25 organizations, RPM for chronic care cut chronic complication admissions by 19%–41%.[45] The other big point is practical: workflow and reimbursement are already in place, so scaling RPM is often more doable than starting from zero.
That’s why RPM works as the baseline non-AI alert model for the comparison below.
Chronic Disease Fit
RPM works best when one simple reading maps to one clear risk signal. Think:
- weight in heart failure
- blood pressure in hypertension
- glucose in diabetes
- oxygen saturation in COPD
In those cases, the model is pretty direct. A post-hospitalization RPM study in CHF and COPD patients found decreased adjusted odds of 6-month mortality and favorable trends across composite outcomes that included death, rehospitalization, and emergency care.[44]
Where RPM starts to strain is multi-signal risk. It can tell you a number crossed a line. What it can’t do as well is sort out why that happened or what’s likely next in the way AI-enabled systems aim to do. RPM still leans on scheduled readings and rule-based escalation, which puts limits on real-time prevention. The next step is to compare this baseline with AI-integrated wearables on speed, accuracy, and actionability.
Head-to-Head Comparison by Criterion
Standard RPM sets the baseline. The table below shows how the other options stack up across the four criteria that matter most in chronic disease monitoring. RPM helps cover the gap between office visits. This comparison shows where each option works well and where it starts to fall short.
| Technology | Timeliness | Predictive Accuracy | Clinical Integration | Chronic Disease Fit |
|---|---|---|---|---|
| AI-Integrated Wearables | Continuous; some systems can flag risk up to 17 hours ahead [48] | Highest - AUC 0.89 and 81.8% accuracy for adverse outcomes [48] | Growing; some clinical-grade devices sync with EHRs and clinician portals [2] | Heart failure, COPD, arrhythmias, diabetes, hypertension |
| Non-AI Wearables | Continuous tracking, but alerts can be delayed or missed if users do not actively engage | Limited; mostly data logging with basic threshold checks | Limited; data often stays in proprietary apps | Mild hypertension and early diabetes |
| Connected Home Medical Devices | Near real time when patients measure on schedule | Moderate; rule-based triggers can create false positives or miss events | Moderate; integration varies by vendor and health system | Hypertension, heart failure, diabetes, COPD |
| Clinic-Based Diagnostics | Low; visit-based snapshots with no between-visit alerts | High at discrete time points; weak for day-to-day risk detection | Highest; embedded in EHR and billing workflows | Best for diagnostic confirmation and complex management |
| Standard RPM Programs | Near real time, but depends on staffing and review schedules | Moderate; threshold-based alerts with some predictive add-ons | Strong; CMS billing codes support structured workflows [46][47] | Heart failure, diabetes, hypertension, COPD |
The biggest split comes down to speed vs. workflow depth. AI-integrated wearables lead on timeliness and predictive accuracy. Clinic-based diagnostics and standard RPM, on the other hand, still have the edge when it comes to clinical integration and clear escalation paths.
That tradeoff shapes the rest of the comparison. One side is faster and more forward-looking. The other fits more neatly into day-to-day care delivery.
Pros and Cons of Each Monitoring Option
Every monitoring option has a strong side and a weak side. What matters in practice is pretty simple: which system spots meaningful change early without flooding people with false alarms.
So this isn’t just a feature-by-feature comparison. It’s a look at day-to-day trade-offs: what works well, where things slip, and what that means for patients and care teams.
| Technology | Key Strengths | Key Limitations |
|---|---|---|
| AI-Integrated Wearables | Predictive alerts for early intervention; personalized thresholds that reduce false positives [6][52][2] | Alert fatigue if thresholds are poorly tuned; accuracy issues from motion artifacts, skin tone variation, or device placement; privacy and cybersecurity risks; battery and connectivity dependence [49][19][55] |
| Non-AI Wearables | Lower upfront cost; good for basic tracking; simpler data sharing [22] | No predictive analytics; generic goals may be unsafe for people with chronic conditions; missed syncs can create data gaps [22][20][19] |
| Connected Home Medical Devices | More accurate for single clinical measurements; fits existing RPM workflows [53][1][3] | Visit-based rather than continuous; depends on proper technique, calibration, and device upkeep; replacement costs add burden; privacy and security concerns remain [53][19][49][55] |
| Clinic-Based Diagnostics | Best for confirmation, not continuous alerting; access to advanced in-clinic testing [50][54] | Visit-based, so changes between visits can be missed; slower and costlier than home monitoring; scheduling and transportation barriers affect many patients [6][39][56][19] |
| Standard RPM Programs | Structured clinical oversight with home data; can improve control and reduce readmissions [53][1][56][57] | Increased care team workload; anxiety from frequent alerts; technology barriers; privacy and security concerns; Medicare data requirements can add compliance pressure [49][50][55][1][39] |
Across almost all of these systems, the same three problems keep showing up: alert fatigue, privacy risk, and alert overload.
Too many notifications, especially false positives, can wear people down. And once patients or clinicians start tuning them out, the problem stops being a minor annoyance and starts becoming a safety issue [49][2][42]. It’s a bit like a car alarm that goes off so often nobody looks up anymore.
Privacy is another weak spot. AI wearables and RPM platforms face steady cybersecurity concerns because data keeps moving all the time. Consumer wearables add a different problem: many users don’t fully realize how much biometric data may be shared with app developers or advertisers [50][55].
What helps most? Personalization and clear escalation paths.
When alert thresholds match a person’s usual range, the system tends to produce less noise. When minor changes are bundled into daily summaries instead of firing off one alert after another, people can focus on what matters. And when patients get direct instructions on what to do after an alert, follow-through tends to improve [51][2][56].
The best systems don’t just send alerts. They turn alerts into clear next steps.
Conclusion
AI-integrated wearable sensors make the most sense when the goal is continuous, personal alerts. They can track heart rate, oxygen saturation, sleep, and activity all day and night, then spot small shifts before they grow into bigger health issues. For heart failure, arrhythmias, and COPD, those early alerts can affect care in a meaningful way. Wearable cardiovascular monitors have shown up to 95% sensitivity and 93% specificity, while prompting clinical changes in up to 35% of cases.[58] That's a strong use case. But it doesn't do the whole job by itself.
Wearables can help with early detection, but diagnosis and major treatment decisions still depend on validated home devices and clinic-based testing. That matters most for blood pressure, ECGs, labs, and imaging. Put simply, the best device depends on what you need it to do.
In practice, the split is pretty clear:
- Use AI wearables for early awareness and habit change
- Use validated home devices for condition-specific measurements
- Use supervised RPM when alerts need to reach a care team
That also makes device validation and data-sharing checks non-negotiable.
Before choosing any device, check FDA clearance or validation, clinician data sharing, and insurance coverage. And if you want help making sense of all that input, one option is pairing the device with an AI coach.
Healify helps turn wearable data, biometrics, and lifestyle data into a clear, personal action plan through its AI coach, Anna.
FAQs
Which chronic conditions benefit most from AI wearables?
AI-integrated wearables are especially useful for diabetes and prediabetes and cardiovascular disease because they support continuous, real-time monitoring and can help flag issues earlier.
They can also help with obesity, mental health disorders, kidney disease, and neurological conditions like Parkinson’s by picking up subtle shifts from a person’s usual baseline. Healify supports this approach with personalized guidance and actionable insights.
How accurate are AI health alerts in real life?
AI health alerts can work well in day-to-day life because they look at your normal patterns, not just broad population averages.
That changes a lot.
Instead of comparing your heart rate, sleep, or other signals to a generic benchmark, the system learns what’s normal for you. From there, it can spot changes that might matter. It also cuts out noise, fixes sensor mistakes, and adds context. For example, a high heart rate during a workout means something very different from a high heart rate while you're asleep.
Results differ from one device to another, of course. But the best way to think about these systems is as early warning tools. They’re not final judges. They help flag patterns sooner, and they tend to get better over time as they use more data from wearables, lab results, and lifestyle metrics.
Do AI wearables replace home devices or clinic visits?
No. AI-integrated wearables do not fully replace clinic visits, but they can change how chronic disease is managed through proactive, around-the-clock monitoring.
Instead of giving only occasional snapshots, these devices provide 24/7 data that can help spot trends, flag risk earlier, and support faster action. That gives patients and clinicians a better view of what’s happening between appointments and can lead to more informed decisions.
In some cases, that kind of steady tracking may also help cut hospitalizations and emergency department visits.