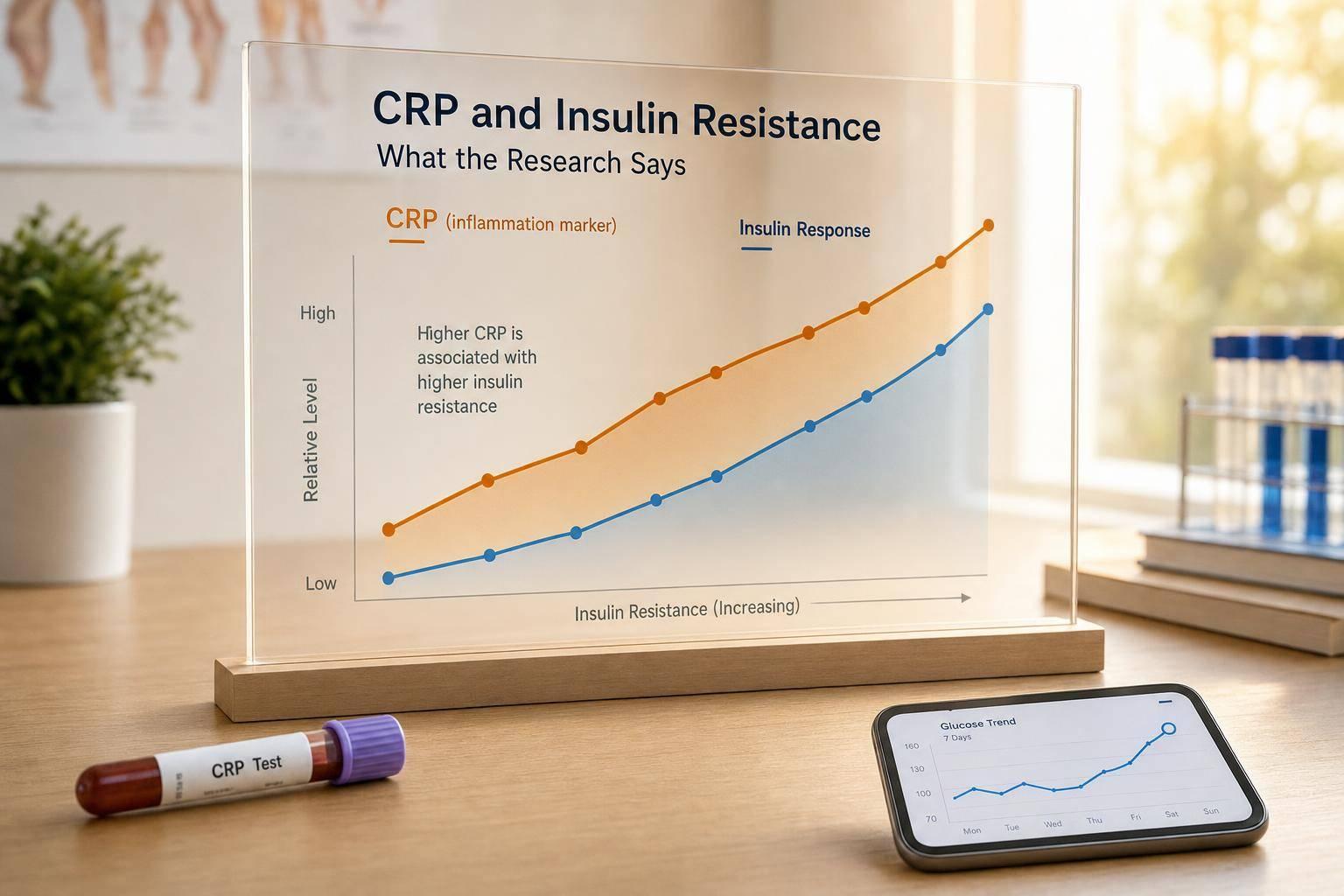
Higher hs-CRP usually shows up with higher insulin resistance - but that does not mean CRP is the cause. Most studies find that people with more low-grade inflammation also tend to have higher HOMA-IR, fasting insulin, or other insulin-resistance markers. One study found 2.46x higher odds of insulin resistance with a high hs-CRP/HDL-C ratio, and another found baseline hs-CRP predicted later HOMA-IR over about 6.8 years.
If you want the short version, here it is:
- CRP is an inflammation marker, not a diagnosis of insulin resistance.
- hs-CRP is the version used for low-grade metabolic inflammation.
- Higher hs-CRP often tracks with higher HOMA-IR, fasting insulin, abdominal fat, high triglycerides, and low HDL.
- Obesity can make this link stronger.
- Most evidence shows association, not cause.
- hs-CRP works better with other markers like fasting glucose, fasting insulin, BMI, and waist size than by itself.
- One isolated result is less useful than trends over time.
A few points stand out from the research:
- In adult studies, higher CRP or hs-CRP often lines up with higher insulin resistance markers.
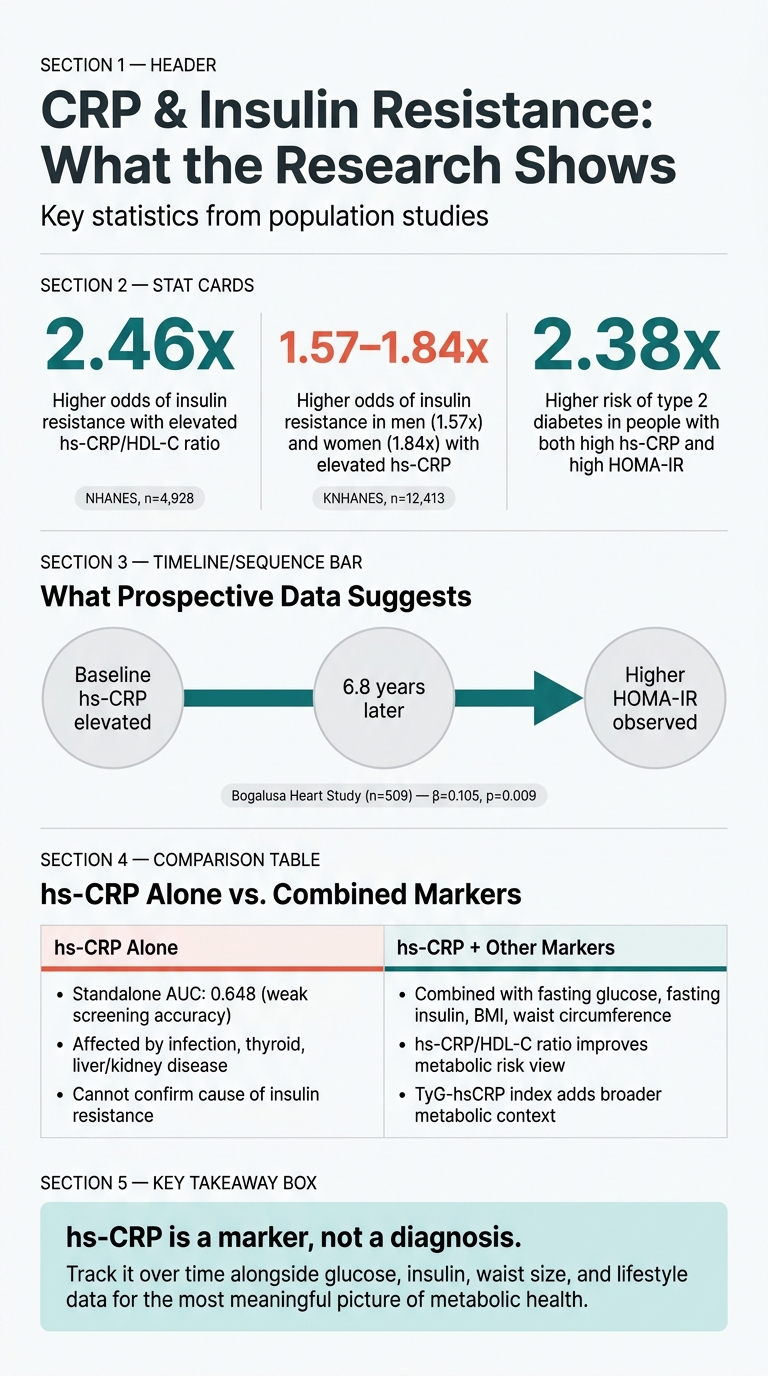
- In one Korean study, elevated hs-CRP was linked to 1.57-fold higher odds of insulin resistance in men and 1.84-fold higher odds in women.
- In one cohort, people with high hs-CRP plus high later HOMA-IR had a 2.38x higher risk of type 2 diabetes.
- hs-CRP alone has limited screening accuracy and can be pushed up by infection, liver or kidney disease, thyroid problems, and other non-metabolic issues.
Bottom line: if you’re looking at metabolic health, I’d treat hs-CRP as context. It can help you spot an inflammation pattern around insulin resistance, but it makes the most sense when you read it next to glucose, insulin, body-size measures, and repeat test results over time.
CRP & Insulin Resistance: Key Stats at a Glance
The Hidden Inflammation Marker That’s Sabotaging Your Metabolism
sbb-itb-f5765c6
How researchers study the CRP-insulin resistance link
Researchers use a few different study designs to look at the CRP-insulin resistance link. Each one answers a slightly different question. Cross-sectional studies show whether two things show up together. Prospective studies are better for checking what seems to happen first.
Cross-sectional studies show patterns, not cause
Cross-sectional studies look at people at a single point in time. The goal is simple: see whether higher hs-CRP tends to show up alongside higher HOMA-IR or fasting insulin. For example, an analysis of 4,928 adults from NHANES found that an elevated hs-CRP/HDL-C ratio was associated with 2.46-fold higher odds of insulin resistance [8].
That kind of result is useful, but it has limits. It can’t tell you what came first - the inflammation or the insulin resistance. It also has to deal with confounders such as BMI, waist circumference, and other metabolic factors. If those aren’t adjusted for, the picture gets muddy. CRP may look tied to insulin resistance when it may just be moving in step with obesity and other metabolic risks. That’s why prospective studies matter.
Prospective studies test whether higher CRP predicts future diabetes risk
Prospective cohort studies follow people over time, so they’re better for sorting out sequence. In the Bogalusa Heart Study, baseline hs-CRP predicted later HOMA-IR, which suggests inflammation may come before insulin resistance in that cohort [2]. Together, hs-CRP and HOMA-IR also improved diabetes risk prediction [2].
Systematic reviews and meta-analyses pool results from many studies to get a steadier read on the overall CRP-insulin resistance link. The table below shows how different study designs shape the evidence.
Study comparison table
| Study | Population | Sample Size | Country | CRP Measure | IR Metric | Key Adjustments | Main Finding |
|---|---|---|---|---|---|---|---|
| Bogalusa Heart Study [2] | Non-diabetic adults | 509 | USA | hs-CRP | HOMA-IR | Race, sex, age, BMI, smoking, alcohol | Baseline hs-CRP predicts future HOMA-IR; joint effect with HOMA-IR improves type 2 diabetes risk prediction [2] |
| NHANES 2015–2018 [8] | Adults with BMI > 18.5 | 4,928 | USA | hs-CRP/HDL-C ratio | HOMA-IR | Age, sex, race, BMI, lipids, blood pressure, smoking | Elevated hs-CRP/HDL-C ratio linked to 2.46-fold higher odds of insulin resistance [8] |
| KNHANES 2016–2018 [4] | Non-diabetic adults | 12,413 | South Korea | hs-CRP | TyG index | Age, smoking, alcohol, activity, blood pressure, lipids | High hs-CRP and high BMI showed a synergistic association with insulin resistance risk [4] |
| CHMS Cycles 1–4 [5] | Healthy adults (no diabetes) | 4,024 | Canada | CRP | HOMA-IR | Sex, age, HDL-C, TG, BMI, smoking, blood pressure | CRP was independently associated with insulin resistance in men, but not consistently in women [5] |
These study-design differences explain why the findings below should be read as associations, not proof of cause. That’s the reason the next section focuses on association rather than causation.
What the research says about CRP and insulin resistance
Adult studies generally find higher CRP linked to higher HOMA-IR
In adult observational studies, higher CRP or hs-CRP is consistently tied to higher HOMA-IR and fasting insulin. Put simply, when CRP goes up, markers of insulin resistance often go up too.
One Korean population study found that elevated hs-CRP was linked to 1.57-fold higher odds of insulin resistance in men and 1.84-fold higher odds in women, even after adjusting for age, physical activity, and lipid levels [4]. That matters because CRP usually doesn’t go up on its own.
Higher CRP also tracks with broader metabolic risk
Higher CRP often shows up alongside abdominal obesity, high triglycerides, low HDL, and higher glucose. So in most cases, it points to a broader metabolic pattern, not one isolated lab value.
That’s why CRP can work as a useful risk signal. It tends to move with the same problems that often sit around insulin resistance. The harder question is timing: is CRP just moving alongside these changes, or can it show up before insulin resistance takes hold?
Association does not prove CRP causes insulin resistance
That link, by itself, does not prove CRP causes insulin resistance. The Bogalusa Heart Study found that baseline hs-CRP significantly predicted HOMA-IR 6.8 years later (β = 0.105, p = 0.009), while baseline HOMA-IR did not predict future hs-CRP [2].
That finding hints that inflammatory stress may come earlier in at least some cases. At the same time, cause and effect are still hard to pin down in humans. Inflammatory cytokines such as IL-6 and TNF-α may disrupt insulin signaling in the liver, muscle, and fat [4][6], but proving that full chain of events directly is tough.
For now, CRP is best viewed as a marker of inflammatory stress. It tracks with insulin resistance in a steady way, but its direct causal role is still not fully settled.
Why these findings matter for metabolic health tracking
Using hs-CRP alongside glucose, insulin, and lifestyle data
CRP is a marker, not a driver. That’s why its main role here is trend tracking.
A1C and fasting glucose show glycemia. hs-CRP adds the inflammation piece those tests don’t show. In some studies, hs-CRP goes up before glucose markers do. And people with both high baseline hs-CRP and high follow-up HOMA-IR had a 2.38 times higher risk of developing type 2 diabetes than people with low levels of both [10].
hs-CRP also helps put body size in context. When you use it alongside measures like waist size or other body-size data, it can help separate inflammatory risk from adiposity alone [4]. In a national study, people in the highest hs-CRP/HDL-C quartile had higher odds of insulin resistance and type 2 diabetes [1].
Put together, these markers show more than any single lab result can. The big idea is simple: watch patterns over time, not one isolated test. hs-CRP is most useful when you follow it across repeat tests and compare it with fasting insulin, waist circumference, sleep, and activity data.
How Healify can support personalized tracking
If you’re tracking these markers over time, Healify can keep everything in one place.
Healify is an iPhone app that brings together bloodwork, wearable data, and lifestyle inputs. It then turns hs-CRP and related markers into personalized guidance through its 24/7 AI coach, Anna.
Limits of the evidence and the main takeaway
Current research limitations
These findings help, but they come with clear limits. The link shows up again and again, yet most of the studies are observational. That means they can show an association, but they can't prove that hs-CRP causes insulin resistance. The reverse may also be true: insulin resistance may help drive inflammation.
So the big question isn't whether hs-CRP matters. It does. The issue is how much weight to give it.
| Limitation | What It Means |
|---|---|
| Cross-sectional study design | Can't show causation [1][3] |
| Unmeasured factors such as diet, exercise, medications, and income can distort results | Effect may be overstated [1][9] |
| Different insulin-resistance measures (HOMA-IR, TyG index) make studies harder to compare | Harder to compare across studies [1][4] |
| Limited standalone accuracy (AUC 0.648) | Weak standalone screen [3] |
| CRP may behave differently by sex and age | May vary by sex and age [9][5] |
Lab methods matter too. Different assay methods and ethnicity-specific cutoffs can shift what counts as "high" hs-CRP from one study to another. In plain English, a high result in one group may not mean the same thing in another. CRP can also go up for reasons that have little to do with metabolic health, including thyroid dysfunction, liver or kidney disease, and acute or chronic infections [1].
Key points to remember
That's why hs-CRP should be read as context, not as a diagnosis. Based on the current evidence, a few points stand out:
- hs-CRP tracks insulin resistance and diabetes risk, but it works best when read with BMI, glucose, and fasting insulin.
- Obesity makes the hs-CRP signal stronger [4].
- Composite markers do a better job than hs-CRP alone. Ratios like hs-CRP/HDL-C or the TyG-hsCRP index give a broader view of metabolic risk [1][7].
FAQs
Can high hs-CRP mean something other than insulin resistance?
Yes. hs-CRP can point to things other than insulin resistance. It’s a general marker of inflammation across the body, not a test that only signals metabolic problems.
Higher hs-CRP is also linked to cardiovascular disease, including heart attack and stroke. And it can go up for other reasons too, especially with inflammatory conditions.
Which labs matter most alongside hs-CRP?
Alongside hs-CRP, the main labs used to assess insulin resistance are fasting insulin and fasting glucose. These two markers are used to calculate HOMA-IR.
A few other markers can help fill in the picture:
- A lipid panel, especially the hs-CRP-to-HDL-C ratio
- Triglycerides and A1C
- NLR and total white blood cell count
BMI is also often tracked to give more metabolic context.
How often should I recheck hs-CRP?
The research here doesn't say how often hs-CRP should be rechecked.
What it does show is a link between CRP/hs-CRP and insulin resistance. That matters, but it’s not the same as giving a testing schedule.
So if you're looking at hs-CRP as part of metabolic risk follow-up, you'd need a specific clinical guideline or study that spells out when to repeat the test. That timing isn't included in the research summarized here.