
If you work with health data, the short answer is this: use tokenization for patient IDs and use encryption for full records, files, backups, and data moving across networks. In healthcare, that split matters because breaches are expensive: the average U.S. healthcare breach cost hit $7.42 million in 2025, and in 2024 there were 725 large health breaches that exposed about 276.8 million records.
Here’s the plain-English version:
- Tokenization replaces a sensitive value, like an SSN or MRN, with a token
- Encryption turns data into unreadable text that only a key can restore
- Tokenization is best for structured fields that teams still need to search, match, or link
- Encryption is best for full files, notes, images, backups, and data in transit
- In most health systems, using both gives better protection than picking only one
This comparison comes down to a few simple questions:
- What kind of data is it? Structured ID field or full record?
- Does it need to move? If yes, encryption is the answer
- Does it need to stay linkable across systems? If yes, tokenization helps
- Do you want less PHI in day-to-day apps? Tokenization can help with that
Bottom line: if you tokenize identifiers and encrypt everything around them, you cut exposure without breaking common healthcare workflows.
Encryption Vs Tokenization | Difference between Encryption and Tokenization
sbb-itb-f5765c6
Quick Comparison
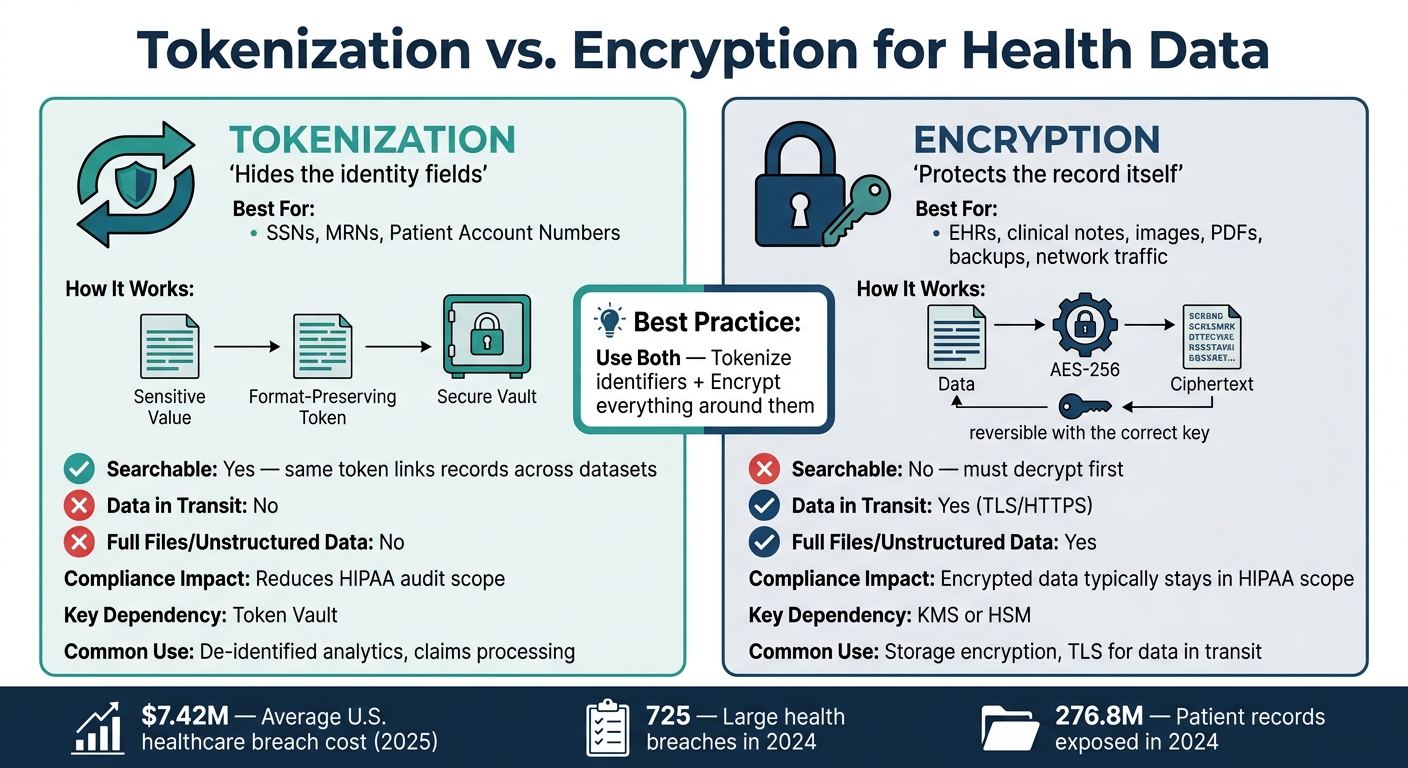
Tokenization vs. Encryption for Health Data: Side-by-Side Comparison
| Criteria | Tokenization | Encryption |
|---|---|---|
| What it does | Swaps sensitive data for a token | Scrambles data with a key |
| Best for | SSNs, MRNs, patient account numbers | EHRs, notes, images, PDFs, backups, network traffic |
| Search and record matching | Good | Often needs decryption first |
| Data in transit | No | Yes |
| Full files and unstructured data | No | Yes |
| Main dependency | Token vault | KMS or HSM |
| Common healthcare use | De-identified analytics, claims IDs | TLS/HTTPS, AES-256 for storage |
I’d sum it up like this: tokenization hides the identity fields, and encryption protects the record itself. That’s the frame I’d use before looking at any tool or workflow.
How tokenization and encryption work
The main difference comes down to how each one is used: tokenization protects specific data fields, while encryption protects full datasets and the connections that move data around.
How tokenization protects structured PHI
Tokenization works at the field level. It swaps sensitive identifiers with tokens. So when an application sends a Social Security number or Medical Record Number (MRN) to a tokenization system, that system creates a replacement value, stores the original in a secure token vault, and sends only the token back to the application. Only approved workflows can turn that token back into the original value through detokenization , which is essential for AI tools for patient-centered treatment plans [6][7].
One big plus is that tokens usually keep the same format as the original data. A 9-digit SSN can be replaced with a different 9-digit number, which means analytics and reporting tools can still process the data without schema changes [5][6].
How encryption protects data at rest and in transit
Encryption turns data into ciphertext using a key. It's used across databases, backups, files, and data moving between systems with algorithms such as AES-256 [7][3].
Encryption is the better fit for unstructured or moving data. Clinical notes, medical images, and full records don't sit neatly inside structured fields, so tokenization doesn't work well for them. Encryption handles those data types and also protects data in transit - like emails, medical device syncs, or patient portal connections - usually through TLS [7][1].
As of January 2025, HIPAA requires encryption as a standard safeguard [3].
Key differences between tokenization and encryption in healthcare
The choice comes down to where data lives, how it moves, and who needs to see it. This is especially critical when using AI tools for biomarker monitoring that handle sensitive health metrics. In healthcare, that can change the whole setup.
| Criteria | Tokenization | Encryption |
|---|---|---|
| Reversibility | Not reversible without vault access; no mathematical link to the original value [4][1] | Reversible with the correct cryptographic key [4][1] |
| Dependency | Requires a secure, central token vault [4][1] | Requires a Key Management System (KMS) or HSM [3][1] |
| Data Format | Preserves the original format (e.g., a 9-digit SSN stays 9 digits) [4][1] | Usually changes format unless Format-Preserving Encryption (FPE) is used [1] |
| Search & Analytics | High; the same token can link records across datasets without exposing identity [2] | Low; data typically must be decrypted before it can be searched [1] |
| Compliance Scope | Can significantly reduce audit scope by removing sensitive data from operational systems [1][8] | Encrypted data usually stays in scope because the sensitive data still exists in the environment [1] |
| Best Fit | Structured PHI: SSNs, MRNs, Patient Account Numbers [1][8] | Unstructured data, files, backups, and data in transit [3][1] |
Where tokenization has the advantage
This gap shows up most clearly in workflows built around structured identifiers. Tokenization’s biggest edge is joinability. When the same identifier maps to the same token, teams can connect records across datasets without exposing identity [2].
It also cuts compliance exposure. If an application only handles tokens, raw sensitive data never shows up in day-to-day systems. That can significantly reduce HIPAA audit scope [1][8].
Where encryption has the advantage
Encryption works best for unstructured data, such as clinical notes, images, and traffic in transit [3][1]. It protects the data around the identifiers, especially when that data moves between systems or sits in storage.
As of January 2025, HIPAA requires encryption as a standard safeguard [3].
Why many health systems use both
In practice, the strongest setup uses tokenization for identifiers and encryption for everything around them. A lot of health systems use both layers together: tokenize the highest-risk structured identifiers - SSNs, MRNs, and Patient Account Numbers - so they never appear in raw form in operational systems, then encrypt the surrounding database, all backups, and every transmission path [1][3].
"Tokenization removes sensitive values from application tiers and shrinks your compliance footprint, but it does not protect the communication channels those systems rely on." - Netwrix Team [1]
That’s the key point. Tokenization helps keep structured PHI out of front-line systems, while encryption protects storage, backups, and transport. The vault should stay isolated, and the keys should stay separate from the data they protect [1][3].
Use cases: which method fits best
These differences show up fast in day-to-day healthcare work. The best method depends on the type of data and what your team needs to do with it. Structured identifiers and unstructured records need different kinds of protection. Get that choice wrong, and you leave holes.
When tokenization is the better fit
Tokenization works best for sensitive data that still needs to stay searchable across systems. In healthcare, that often means Social Security Numbers, MRNs, and Patient Account Numbers inside claims systems. A billing team can process a claim with a token that looks like the original ID, without handling the actual value.
It also works well for analytics on de-identified datasets. Say a population health team needs to track patient outcomes across lab systems and claims data. Tokens keep records linked without exposing PHI. That means teams can connect lab and claims records while keeping identity out of view.
There’s one catch: this is for structured fields. It does not fit files or live traffic.
When encryption is the better fit
Encryption is the right fit for full records, files, and anything moving between systems. Clinical notes, DICOM images, PDF lab reports, and full EHR records need encryption, not tokenization. AES-256 handles that kind of data well and does not need the data to match a specific format.
Any data in transit, like wearable syncs, API traffic, or provider messaging, should use TLS or HTTPS. Tokenization can protect single data elements at rest, but it does not protect the channel carrying that data. A wearable app, for example, depends on transport encryption to keep data safe as it moves from device to server.
That’s the basic rule for anything in motion or stored as a full record.
A simple decision rule for health data teams
Use encryption for full records and traffic. Use tokenization for identifiers and linkable fields. If both apply, tokenize the identifier and encrypt the file.
"Tokenization delivers the greatest value when sensitive data needs to be stored or referenced but rarely processed in its original form." - Netwrix Team [1]
Use case comparison table
| Use Case | Tokenization | Encryption | Best Use |
|---|---|---|---|
| Patient identifiers in claims systems | Yes - format-preserving token replaces ID | Possible, but changes format | Tokenization |
| Full EHR records / clinical notes | No | Yes - AES-256 handles efficiently | Encryption |
| Wearable device data sync | No | Yes - TLS 1.3 secures data in motion | Encryption |
| Lab PDFs and images | Can tokenize specific fields only | Protects the entire file at rest | Encryption |
| API traffic / data in motion | Protects elements within the payload | Secures the full transmission channel | Encryption |
| Analytics on de-identified datasets | Yes - maintains record linkage without PHI | No | Tokenization |
| Cloud storage backups | No | Yes | Encryption |
Conclusion: Layered protection is usually the safest choice
After looking at where each method works best, the practical rule is pretty simple: tokenization and encryption do different jobs. Encryption protects records and data moving across networks. Tokenization strips high-risk identifiers out of day-to-day systems, so if a database is breached, the attacker sees tokens instead of the original values.
Use both. Tokenize high-risk identifiers in apps, and encrypt the transport, token vault, databases, and backups. That mix cuts the blast radius if something goes wrong.
The same idea carries over to modern health apps and hospital systems. Apps that combine wearables, biometrics, and lifestyle data need tokenization for identifiers and encryption for data in motion and at rest.
Key takeaways
Start with the data type. A good rule of thumb:
- Tokenize structured identifiers
- Encrypt full records and anything in transit
- Use both when both risks are in play
FAQs
When should I use both tokenization and encryption?
Use both when you need stronger protection for different types of health data across its lifecycle.
Tokenization is a better fit for structured data, like patient IDs or medical record numbers. Encryption is a better fit for unstructured data and data in transit.
Using both gives you a layered setup that helps protect sensitive identifiers, secure data during transmission and storage, and support HIPAA compliance.
If a breach happens, the exposed data is far less useful without the secure vault or decryption keys.
Does tokenization reduce HIPAA compliance scope?
Yes. Tokenization can cut down HIPAA compliance scope by swapping sensitive patient data for non-sensitive tokens kept in a secure vault.
That means only the vault, and the systems that connect to it, usually stay in scope. By contrast, encrypted data is still considered PHI, so systems that handle it generally still fall under HIPAA.
Can encrypted health data still be searched or matched?
Yes, but usually only after decryption.
Encryption turns health data into unreadable ciphertext. So if you want to search it or match it, you often need the decryption key first. That creates a security risk if the key gets compromised.
With tokenization, the original data is swapped out for tokens. Search or matching then depends on access to the secure vault and the detokenization process instead.